What do current treatments for Asthma do?

How PAR-2 affects asthma
PAR-2 expressed on airway epithelial cells mediates the initial inflammatory responses to proteases, released from common household pathogens, including production of cytokines and chemokines; mast cell degranulation; impaired epithelial barrier function and mucus production. Locally released proteases can activate PAR-2 on inflammatory cells (eosinophils, lymphocytes and neutrophils), to enhance chemokine-induced recruitment to the airway and exacerbating the inflammation. Ultimately, thickening of the bronchial epithelium and secretion of mucus causes obstruction of the airways and bronchoconstriction.
What is our approach to Asthma involving PAR-2?
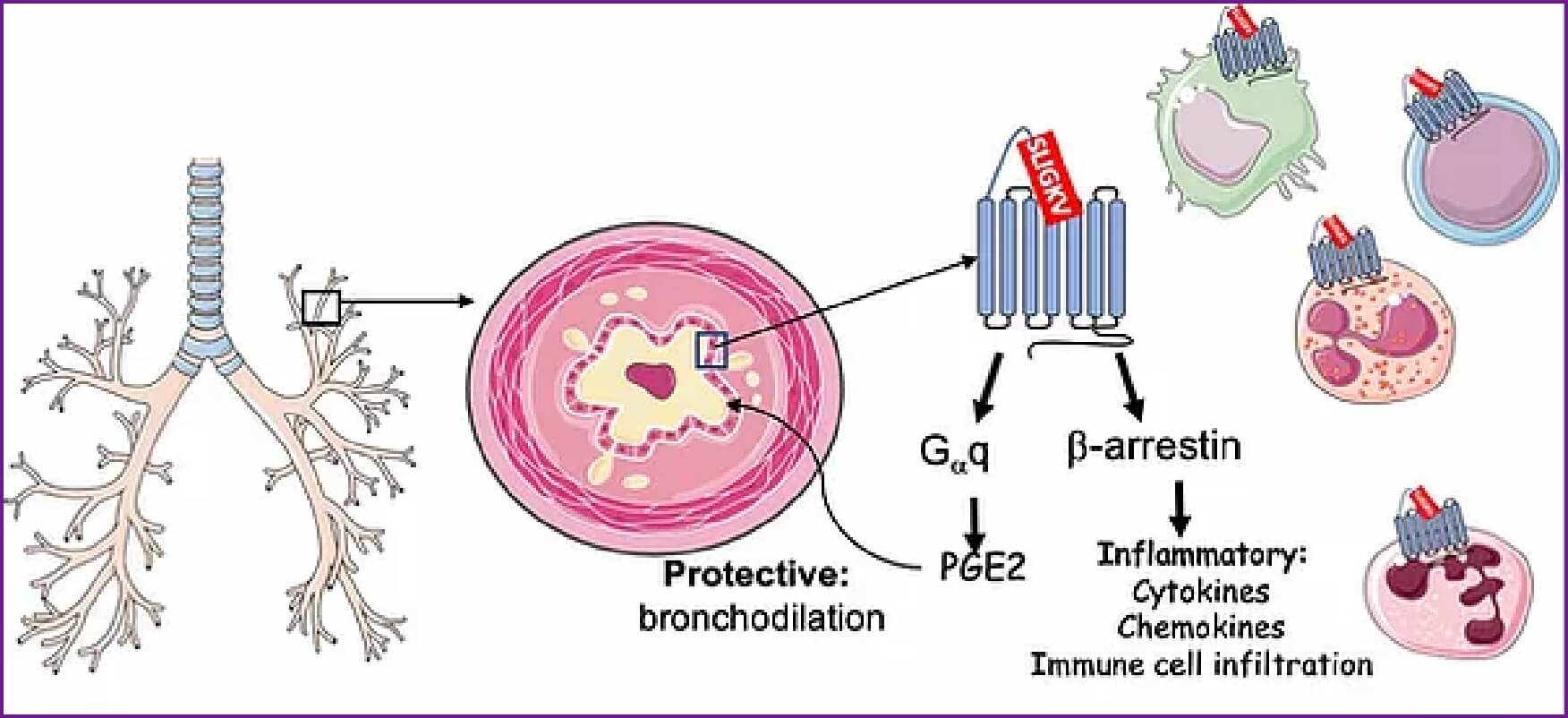
Previous attempts to pursue PAR-2 as a therapeutic target for asthma have been difficult because its activation also leads to release of Prostaglandin E2 (PGE2) from epithelial cells, which play a protective role in the airway by promoting smooth muscle relaxation and subsequent bronchodilation. In Alternaria and Cockroach-induced asthma, as well as PAR-2 induced exacerbation of Ova-induced asthma, the inflammatory phenotype is dependent upon signaling through a protein called beta-arrestin, while the protective bronchodilation occurs through a G-protein-dependent pathway. Beta-arrestin-2 recruitment to PAR-2 is required for production of inflammatory interleukins (IL-4, IL-6 and IL-13), mucus production and bronchoconstriction. Expression of beta-arrestin in leukocytes is required for both PAR-2 and chemokine-induced recruitment to the airways. PGE2 production is dependent upon G-protein, but not arrestin signaling. Our approach exploits these distinct signaling pathways to develop PAR-2 antagonists that target the beta-arrestin pathway for the treatment of asthma.


